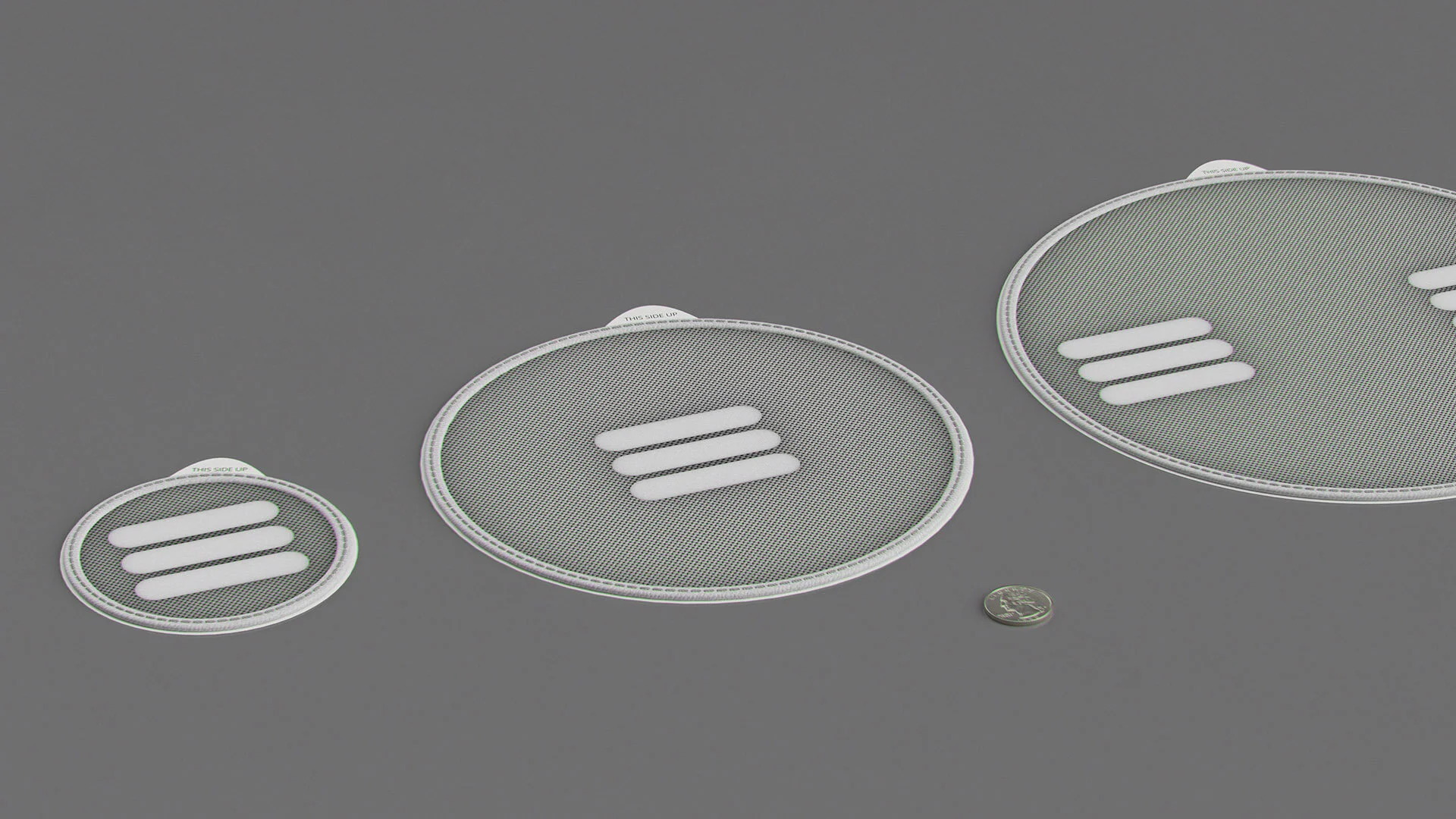
RE°FLEX Nodes: customized skins provide a personalized touch to the experience for PT patients.
“THE BODY DOESN’T WALK BY ITSELF.”
ABOUT
In the context of COVID-19, how might we provide a better remote interaction experience for physical therapists and patients sheltering at home? How might we create meaningful interactions, both on and off the screen? How might we leverage gameplay to motivate daily engagement? How might we receive and transmit physical sensations between people? These and many other questions formed the basis of our design process and research.
OUR SOLUTION
RE°FLEX IS A MULTIMODAL INTERACTION SYSTEM DESIGNED TO ENHANCE LIVE REMOTE COLLABORATION AND COMMUNICATION BETWEEN PHYSICAL THERAPISTS AND THEIR PATIENTS
The goals for this project included:
Exploration: investigate human needs through research, interviews, and evaluation of works by other practitioners.
Synthesis: distill research insights to identify design opportunities and produce a set of criteria.
Iterative design: create representations and artifacts of potential solutions, prototyping toward a refined concept.
This project was collaboration by Yueru Deng, Matt Geiger, Lulin Shan, and Catherine Yochum. in Interaction Design Studio, taught by Kyuha Shim and Dina El-Zanfaly at the School of Design, Carnegie Mellon University.
RE°FLEX combines a variety of technologies: mobile apps, data analytics, smart wearables, and video teleconferencing.

Project Context:
6 weeks
MPS/MDes Interaction Design Studio
CMU School of Design, Fall 2020
Collaborators:
Catherine Yochum
Lulin Shan
Matt Geiger
Yeuru Deng
My Roles:
Product Designer
UX Researcher
Motion Designer
Physical Computing
Industrial Design
3D Modeling
Digital Prototyping
Tools:
Figma
Miro
Photoshop
After Effects
Illustrator
Fusion 360
Maya
Aero
1. Identifying the problem: Moments of Mismatch


Interviewing stakeholders revealed several challenges, as well as viable opportunities for improvement
Video calls: this mode of communication provides some aspects of face-to-face communication, but lacks subtle queues such as eye contact, directed speech, and a sense of space. While this medium works fairly well for one-on-one communications, it begins to lose clarity and effectiveness when used for larger groups.
Body language: webcam and video teleconference systems were designed to facilitate remote meetings, where most body language happens from a seated position. The optics in webcams are usually mounted on or integrated above computer displays. This design is intended to work for subjects who are sitting within arm’s reach of their device. Physical activity requires greater distance.
Touch: sports training, martial arts, physical therapy—these kinds of activities engage our tactile senses. The lack of touch and physical interaction over video conferencing systems is a major obstacle for physical therapy in a remote context. We explored haptics and mixed reality technologies as possible interventions.
2. THE CURRENT STATE: Existing Technologies
A collection of examples found during our design research.
Many remote interaction technologies are designed to address a specific scenario (or a narrow set of scenarios). Considering the scenarios described by our interviewees, we evaluated existing technologies to identify opportunities for improved remote interactions.
To provide meaningful interactions between the physical therapist and patients, we considered a range of platforms and technologies. From our research and interviews, we found a need for better representation of touch beyond vibrating motors.
3. Ideation: User Needs
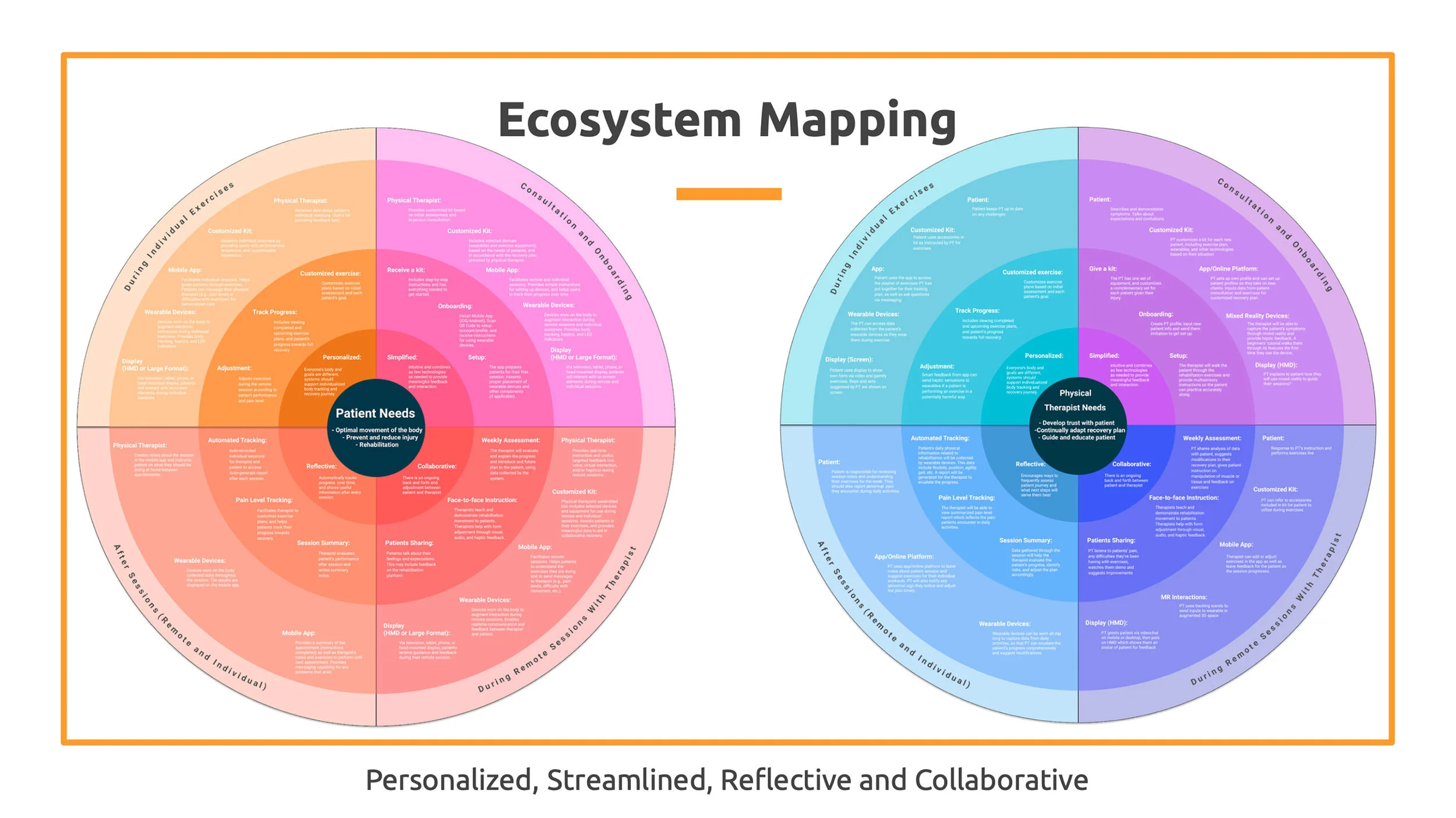
Interviews helped us to understand the needs of physical therapists and their patients, and our ecosystem mapping helped us to understand the relationships between those needs.

Mapping interactions helped our team to establish goals while ideating.

Journey mapping helped us to anticipate user needs.

Prototyping
Physical artifacts and evaluations
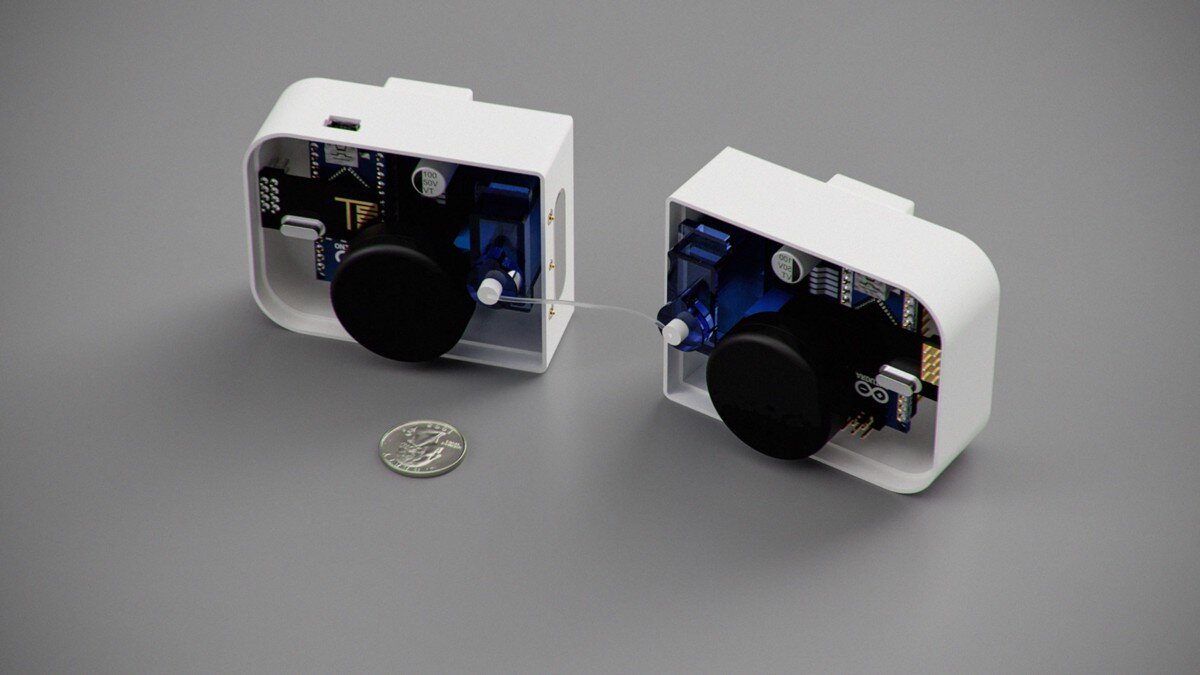
Rendering of proposed physical prototype based on Arduino controlled actuators and nylon filament.

Rendering of clip-on design chassis for potential physical prototype (US quarter included for scale).
We considered using independent servo motors connected by high strength nylon filament (i.e., fishing line) to recreate the feeling of pulling. This mechanism would be capable of wirelessly transmitting gestures for pose and form corrections. While not intended for a final end-user product, this approach helped us to consider other ways to include directionality to remote tactile feedback.

Concept rendering: haptic array to add directional tactile feedback

Figure model by mcramblet, design by Matt Geiger.
Catherine Yochum, demonstrating patient interaction experience with RE°FLEX.
To grapple with the complexity of this large problem space, we decided to narrow our focus onto knee injuries and recovery. In our second pass of prototyping, we envisioned an intelligent knee-brace that could capture real-time movement data, and provide targeted haptic feedback to patients. This approach involved the use of embedded LRA (linear Resonant Actuators) devices and accelerometers. The placement of devices above and below the knee would allow for directional and three-dimensional haptic feedback to patients.
As we continued to explore this problem space, including additional interviews, we found that seamlessness is an important consideration. Bulky devices allow for including more robust features and integration, but at the cost of simplicity and wearability. This is an extraordinary drawback for patients who may desire an all-day wearable device, or something that can fit underneath their clothing.
For considerations of a 3rd-generation device, we focused on simplifying the placement and application of devices as well as scalability. The initial question for this pivot in form was: how big is too big? Our second question: how small, and where on the body? While our consideration of a knee brace offered some flexibility, the use of a more modular system presents a much wider range of options. Physical prototyping and evaluation helped to narrow the scope. This evaluation suggested that the dimensions for the adhesive patches needs some revision to operate well on this region of the body. The ultimate goal is to design nodes that are exactly as small as they need to be, but no smaller. The lower limit is critical.

Left: 3M post-it (~3x3"), US postage stamp (featuring American astronaut, physist, and pioneer for women in space, Sally Ride!). Right: postage stamp vs. 1" diameter blue sticker.
Generally speaking, the point of prototyping is to show and tell. Show: what you have in mind, and tell: what that would be like. This process revealed a narrow range of acceptable sizes for nodes (devices combining motion tracking and haptic feedback). These constraints also provided some much needed priorities. Wearable devices are limited by battery capacity, weight, and size. What can be achieved within these limitations matters.
Another consideration: based on feedback we received from physical therapists, it became clear that we needed to design a system with components that differ between the patient and therapist experience. These stakeholders have different needs, and we envisioned a bigger technology investment (into things like a Mixed Reality headset) would be beneficial to the physical therapists. On the patient side, the Reflex Nodes must provide a layer of guidance, adding a felt sense to augment the visual and verbal instructions from the physical therapist.